Glioblastoma Multiforme (GBM) is the most common and most lethal primary malignant brain tumour in adults, with a median survival of only 12-15 months after diagnosis and a five-year survival rate below 5%. Over the past four decades, the standard treatment regimen has undergone virtually no fundamental change -- surgical resection, temozolomide chemotherapy, and radiotherapy remain the core of the Stupp protocol. However, in the first half of 2026, breakthrough advances along three distinct technological routes emerged simultaneously, potentially signalling a turning point in the GBM treatment paradigm.
Route One: EnGeneIC's Targeted EDV Nanocells
In April 2026, Australian biotechnology company EnGeneIC announced the initiation of a Phase I clinical trial in the United States for patients with recurrent GBM. Its core technology platform -- the EDV (EnGeneIC Dream Vector) nanocell -- attracted widespread attention from both academia and capital markets. Shortly thereafter, in June, EnGeneIC received the 2026 Breakthrough in Glioblastoma Biotech Award, jointly presented by the Northwell Foundation and Lenox Hill Neurosurgery.
The working principle of EDV nanocell technology is unique: nanoscale (approximately 400 nm) cell vesicles extracted from Escherichia coli, genetically engineered to express targeting antibody fragments against the EGFR receptor on their surface, are loaded internally with high-concentration chemotherapeutic drugs. Because GBM cells universally exhibit high EGFR expression, EDV nanocells can specifically deliver chemotherapy drugs to tumour tissue while avoiding systemic toxicity.
The key breakthrough of this technology lies in overcoming the blood-brain barrier (BBB), the fundamental obstacle to GBM chemotherapy. Traditional chemotherapeutic agents such as paclitaxel and doxorubicin, while cytotoxic to GBM cells, cannot effectively cross the BBB. Thanks to specific surface modifications, EDV nanocells can traverse the BBB via receptor-mediated transcytosis, delivering drugs directly to intracranial tumours.
EnGeneIC has already planned to initiate a Phase IIa clinical trial in the United States and is in discussions with the FDA regarding the possibility of accelerated approval. Initial Phase I data show that EDV nanocells exhibit a favourable safety profile in patients with recurrent GBM, with some patients demonstrating preliminary efficacy signals of disease stabilisation.
Route Two: University of Cincinnati Nanofiber Multidrug Delivery System
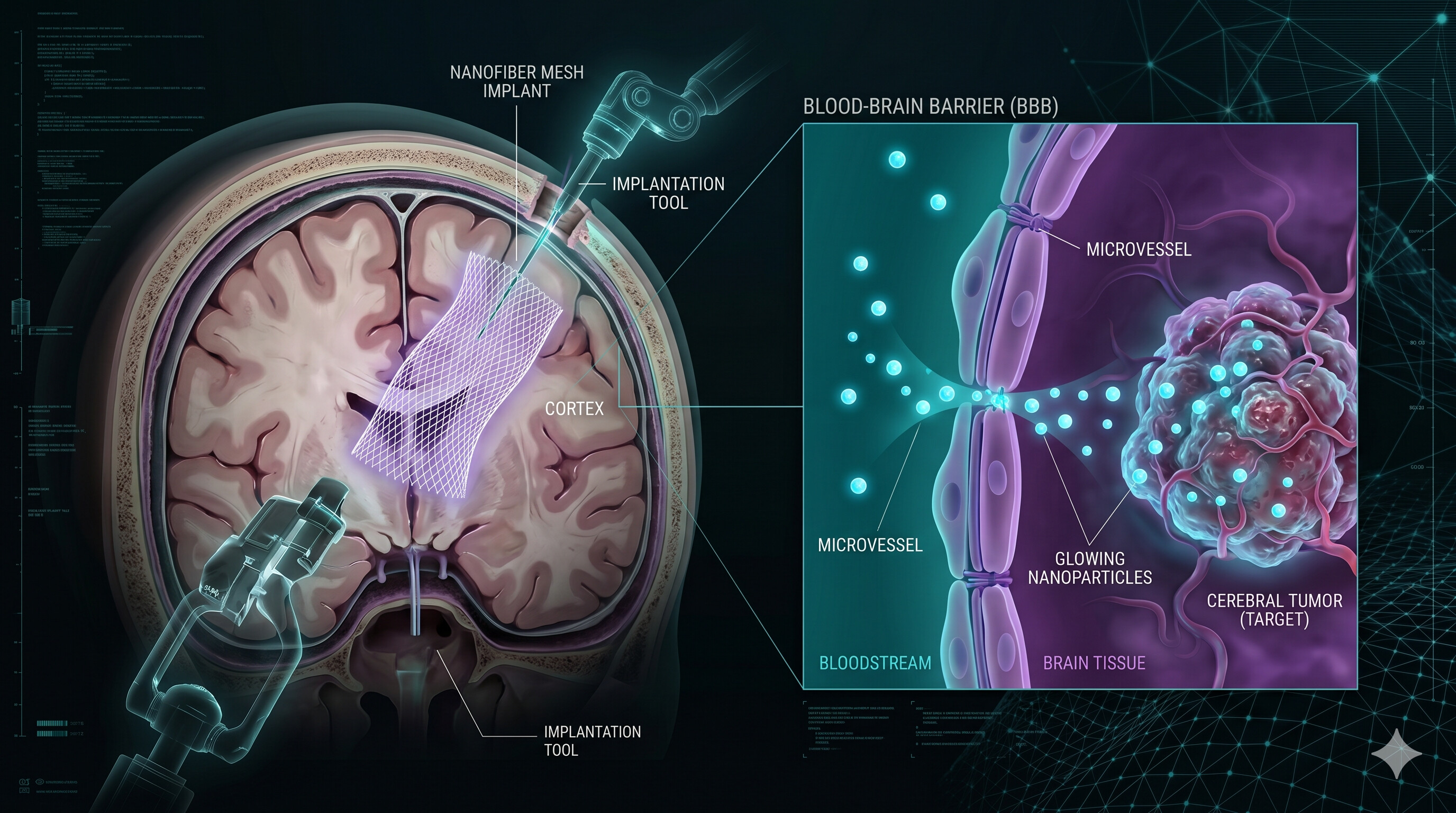
In June 2026, a joint research team from the University of Cincinnati and Johns Hopkins School of Medicine published a breakthrough study in Nature Communications: an implantable nanofiber mesh capable of sustained local release of multiple chemotherapeutic drugs postoperatively, acting directly on residual tumour areas following surgical resection.
The engineering core of this technology lies in the nanofiber matrix prepared by electrospinning. The research team used biodegradable polymer (PLGA) as a carrier to embed three chemotherapeutic agents with distinct mechanisms of action -- temozolomide, panobinostat, and a novel HDAC inhibitor -- into the fibre structure. By modulating the polymer degradation rate, the nanofiber mesh can continuously release drugs over 3-6 weeks post-surgery, covering the most dangerous early recurrence window after GBM resection.
In preclinical animal models, GBM-bearing mice treated with the nanofiber mesh exhibited a median survival extension of more than 80%, with some mice achieving long-term tumour-free survival. Histological analysis revealed that the nanofiber mesh formed a high-concentration drug gradient around the implantation site, effectively killing residual tumour cells at the surgical margin. Meanwhile, because the drugs are released locally rather than systemically, systemic toxicity was markedly reduced.
Another innovation of this technology lies in its tunability. By adjusting the ratios of different polymers and the fibre diameter, the research team can precisely control the release kinetics of each drug, achieving a sequential chemotherapy regimen along the time dimension. For example, a DNA alkylating agent (temozolomide) can be preferentially released in the first postoperative week, then switched to a histone deacetylase inhibitor (panobinostat) in the second to third weeks to maximise synergistic cytotoxicity.
The research team plans to submit an Investigational New Drug (IND) application to the FDA in 2027 and initiate human clinical trials.
Route Three: University of Alberta GBM Invasion Mechanism and Therapeutic Target
In June 2026, the Experimental Oncology research team at the University of Alberta in Canada published a major discovery concerning the mechanism of GBM spread, identifying a potential therapeutic target in the process. The study revealed the molecular mechanism by which GBM cells undergo aggressive invasion along white matter fibre tracts -- the very reason GBM is termed "multiforme" and why complete resection is so difficult.
The research team found that an adhesion molecule named AMIGO2 is significantly overexpressed in invasive GBM cells. AMIGO2 regulates the adhesion strength between cells and the extracellular matrix, enabling tumour cells to migrate along blood vessels and nerve fibre tracts. In animal models, silencing AMIGO2 expression using RNA interference technology reduced tumour cell invasive capacity by approximately 70%, and overall survival in mice was significantly prolonged.
The clinical value of this discovery lies in the potential utility of AMIGO2 as a biomarker for postoperative GBM prognosis -- patients with higher levels of AMIGO2 expression in tumour tissue face a greater risk of early postoperative recurrence. Meanwhile, targeted therapeutic strategies against AMIGO2 (including monoclonal antibodies and small-molecule inhibitors) have already entered the lead compound optimisation phase.
The Alberta team emphasised that, unlike traditional cytotoxic chemotherapy, treatment targeting the tumour cell infiltration mechanism does not directly kill cells but rather prevents their spread. This shifts the biological behaviour of the tumour from diffuse invasion to localised growth, which is far more manageable within the coverage scope of surgery and radiotherapy.
Synergistic Prospects of the Three Routes
These three technological routes are not competing with one another; rather, they form a natural synergy at different stages of GBM treatment:
EnGeneIC's EDV nanocells provide a systemic targeted treatment modality suitable for GBM patients with multifocal lesions or diffuse infiltration. They can be used as neoadjuvant therapy before surgery or as adjuvant therapy after surgery.
The University of Cincinnati's nanofiber mesh targets the central pain point of GBM treatment -- local recurrence at the surgical site. More than 90% of GBM recurrences occur within 2 centimetres of the primary lesion. Implanting the nanofiber mesh immediately after surgical resection establishes a local drug concentration barrier, preventing the growth of microscopic residual tumour cells.
The University of Alberta's AMIGO2 targeting strategy, meanwhile, addresses the root of tumour biology, limiting the invasive capacity of GBM cells and fundamentally reducing the risk of GBM recurrence. If combined with the local chemotherapy of the nanofiber mesh -- the former controlling distant tumour infiltration and the latter eliminating microscopic residual at the surgical margin -- it may achieve three-dimensional control over GBM.
Observatory Analysis
GBM is called the "king of cancers" for two core biological challenges: tumour heterogeneity and diffuse infiltration. The three technological routes that emerged in the first half of 2026 address these two challenges from different angles -- EDV nanocells tackle heterogeneity through targeted delivery, the nanofiber mesh addresses infiltration through sustained local drug administration, and the AMIGO2 target severs the infiltration signalling pathway at the molecular level.
It is worth noting that all these technologies are at a very early stage. EnGeneIC is still in Phase I/II trials, the nanofiber mesh remains in the preclinical stage, and the AMIGO2 target is still years away from entering the clinic. However, viewed through a historical lens, the GBM field has seen numerous Phase III trial failures over the past decade (including negative results for bevacizumab, cediranib, and several other drugs). The emergence of new technological routes is itself a positive signal for the direction of research.
For the Chinese and Asian healthcare ecosystem, the cost of precision GBM treatment is a critical issue. The production cost of biologics such as EDV nanocells is far higher than that of traditional chemotherapeutic drugs. Without medical insurance coverage, patient out-of-pocket costs could exceed US$50,000-100,000 per treatment course. Pricing and accessibility will be unavoidable challenges in the commercialisation of these technologies.
Overall, 2026 marks a shift in GBM treatment from the traditional "one drug fits all patients" model towards a tripartite, three-dimensional treatment strategy of "precision targeting, local drug delivery, and infiltration control." Although a true cure remains a long way off, this is the most encouraging moment the GBM research field has seen in years.
Disclaimer: This article is for informational purposes only and does not constitute investment advice. Data and timestamps are accurate as of the publication date and may change with subsequent developments. Neither the author nor POC.HK assumes any liability for losses arising from the use of this information.